
Writing By Gia Miller
Artwork by Justin Negard
When Bedford resident Katelyn DiFede was 17 years old, her mother, Janine McEneaney, rushed her to the emergency room six times over the course of seven weeks. Initially, DiFede was treated for an allergic reaction, and once that healed, other urgent and concerning symptoms, such as ovarian cysts, appeared. They became “regulars,” and every trip, even the time DiFede experienced sudden numbness in her arms and legs and couldn’t stand or walk, ended with a similar response: “She’s fine. Go home.”
“It got to the point where our insurance company actually told us they’re not paying anymore,” says McEneaney. “They told me we were being ridiculous, and they asked me why we kept running to the emergency room when there was nothing wrong with her.” But DiFede wasn’t faking it. Every symptom was real. Doctors just didn’t believe her.
In between trips to the ER, DiFede saw a dermatologist. “I started getting acne out of nowhere,” she remembers. “They gave me antibiotics for the acne, and then I started losing my vision. The dermatologist’s office told me that the antibiotic can pinch a nerve in the back of my eyes, so they sent me to the ER.”
“Her vision was going in and out,” McEneaney adds. “She would see some light, and then she’d be blind again. I rushed her to the emergency room. What else could I do? My kid was going blind. That doctor told me he didn’t know what was going on with her, but he asked for my consent to do a spinal tap. He explained that he needed to relieve the pressure in her brain because otherwise, she could be blind forever. So, I agreed. After the spinal tap was complete, they told me her pressure was fine.”
DiFede was sent home. Once again, they told her nothing was wrong. “And then, a couple weeks later, they called to tell me I had Lyme disease in my spinal fluid. But they told me it was probably old Lyme disease from when I was a kid. They gave me two weeks of antibiotics just in case and said I would be good after that.”
When the antibiotics were complete, DiFede still wasn’t feeling well, but she says, “it was not bad enough to go to the emergency room. At that point, I decided I shouldn’t even bother going to the emergency room because they did something as serious as a spinal tap, and they still told me nothing was wrong. So clearly, nothing was wrong with me.”
Instead, McEneaney took DiFede to the pediatrician. “The pediatrician told me, ‘You should admit yourself, because you’re insane. There’s nothing wrong with you,’” DiFede remembers. “So I said to my mom, ‘Okay, I’ll go.’ McEneaney didn’t want her to go, but she let her daughter self-admit. And that’s when everything changed.
DiFede admitted herself to Four Winds, submitting all of her medical records. The next morning, a psychiatrist who worked there one weekend a month reviewed the new patients’ files and noticed the spinal tap. “She walked into my room and said, ‘This isn’t a mental health condition. If you have Lyme disease in your spinal fluid, you have Lyme disease, and that’s what’s causing everything.’ She then told me she studied under a Lyme-literate doctor, and she explained that anxiety, depression, OCD—everything I was experiencing was consistent with Lyme disease. She told me I didn’t belong at Four Winds, and I needed to see a Lyme-literate doctor.”
Finally, years of symptoms made sense. From a likely incorrect diagnosis of Bell’s Palsy when she was five years old to high fevers and a recurring rash throughout childhood, to instant and unexplained severe anxiety and OCD in middle school and extreme sensitivity to light and loss of appetite in high school — they were all symptoms of chronic Lyme disease (CLD). DiFede wasn’t, as her pediatrician suggested, insane. She was suffering from a condition few doctors know how to diagnose or treat.

Katelyn DiFede.
Understanding Lyme disease
In late 1975, two mothers from Old Lyme, Connecticut, were desperate. Their families, along with others in their town, were struggling with an outbreak of both adult and juvenile arthritis that featured several unexplainable symptoms. The women contacted the Connecticut State Department of Health and the Yale School of Medicine, hoping for answers. Dr. Allan C. Steere, a first-year rheumatology fellow at Yale University, and Dr. Stephen E. Malawista, head of the rheumatology section at Yale, along with two doctors from the state, took on the case.
Steere and Malawista began examining patients and interviewing them about their symptoms. One-quarter of the patients studied reported a skin lesion with an expanding bull’s-eye pattern four or more weeks before arthritic symptoms began. They also learned all patients lived in the rural wooded areas of town, the majority of patients first experienced symptoms between June and September, and more. They named the condition Lyme arthritis, and as early as 1976, they believed the tick was what transmitted the disease to humans.
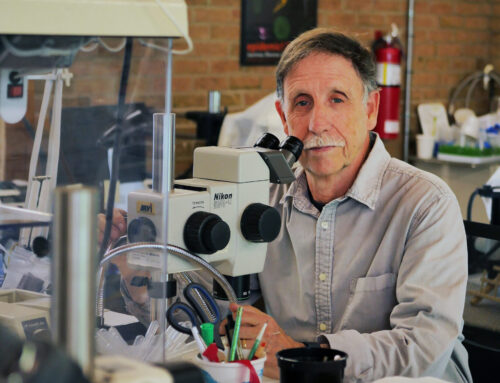
“When Steere discovered the disease, he actually believed it was a chronic infection,” says renowned Lyme disease expert Dr. Richard Horowitz, who has treated Lyme disease patients throughout the U.S., Canada and Europe for almost 40 years. “But because he was a rheumatologist, he started talking about Lyme’s autoimmune phenomena instead.”
Lyme disease, the most common vector-borne illness in the United States, is caused by a spirochete bacteria called Borrelia burgdorferi (B. burgdorferi), which is transmitted through a blacklegged tick. If you know you’ve been infected, treating it immediately is the best course of action. “If you see that bullseye rash, you definitely want to get antibiotics early on,” says Horowitz. “You can usually cure the Lyme at that point in time; between 80 and 90 percent of cases are cured if treated immediately.” Unfortunately, not everyone experiences the bullseye rash or knows they’ve been bitten/infected. Pound Ridge resident Dina Miller (no relation to the author), a retired police detective and yoga instructor, believes she was bitten about 10 years ago, but there is no way to know for sure. “About three years ago, I started developing arthritis,” she remembers. “It was in my hands, and it was really horrible. I also began experiencing general malaise and chronic headaches. I went to the doctor, and they told me nothing was wrong with me.”
“My arthritis got worse, and I began to experience general fatigue and migrant pain,” Miller remembers. “I would have the worst pain—a throbbing, burning pain—in my shoulder one day, and then the next day it would move to my left foot. It constantly moved, and it made me wonder if I was lying about the pain. It felt like my body was gaslighting me. Every time I went to a doctor, they would say, ‘We can’t find anything wrong.’”
Even without the trademark rash, the B. burgdorferi can take hold and secretly damage the body. In 2022, researchers at the Johns Hopkins Institute for NanoBioTechnology learned that once inside the body, B. burgdorferi uses “tenacious trial-and-error movements to find and slip through tiny openings called junctions in the lining of blood vessels near the original bite site. This allows them to hitch a ride on the bloodstream throughout the body, potentially infecting other tissue and organs.” If B. burgdorferi doesn’t immediately succeed, it tries again, continuing to look for an entry until one is found. “The bacteria spend an hour or two using this behavior to find their way into the blood vessels, but once there, they are in circulation in a matter of seconds.” From there, bacteria latch onto various tissues, joints and major organs. They can also penetrate the blood-brain barrier, triggering inflammation in the brain as well as interrupting the communication between nerve cells, which can lead to changes in how the body perceives pain as well as affect a person’s emotional and cognitive functioning. Horowitz says that approximately 90 percent of people struggling with CLD have neurological symptoms. In fact, the two women I spoke with both struggle with brain fog. During our interviews, they needed to pause or refer to notes to remember certain parts of their story.
Without treatment, problems persist, and they can be debilitating. Prior to CLD, Miller lived a very vibrant life. She loved her fast-paced, action-packed job as a police detective in Bridgeport, CT. She investigated, visited crime scenes and spent time working undercover. And as one of three women in the 50-person detective bureau, she held her own. “I was really outgoing, funny, quirky and quick with a joke,” Miller says. “I loved adventure. I would go scuba diving, I ran over 60 miles a week, and I participated in endurance sports.” By the time her first Lyme symptoms appeared, Miller had retired from the force and was a top-rated yoga instructor at Lifetime Fitness in Chappaqua.
But as the disease progressed and Miller’s attempts to receive a proper diagnosis failed, she got worse. She taught 12 to 15 yoga classes a week, and after teaching back-to-back classes, Miller was so exhausted that she slept the rest of the day. “One day at work, I began running a fever,” Miller remembers. “I drove home, and once I lay down, I couldn’t lift up my head; it was killing me. My fever increased to about 103° or 104°, so I was taken to the walk-in medical clinic, where they told me, ‘We think you have sepsis.’ They sent me to Northern Westchester Hospital. I later went into septic shock and ended up in the ICU for four days.”
DiFede’s and Miller’s experiences with multiple doctors, trips to the hospital and false or no diagnoses are common. In Horowitz’s clinic, the Hudson Valley Healing Arts Center, his patients tell the same story. “We have a lot of people who have been to 10, 20 or 30 doctors,” he says. “The largest number I’ve heard of was 100. Years ago, I had a patient who saw 100 doctors before seeing me.”
It’s not only Lyme
“Part of the reason it confuses so many people is they’re not just sick from Lyme,” Horowitz explains. “They’re also sick from other co-infections, like Babesia, which is a malaria-like parasite; I see that in 80 to 90 percent of my patients. Another co-infection is Bartonella, initially known as Cat Scratch Fever, which has 18 different forms; that also shows up in a large number of people whose immune system has been affected. Additionally, mold, toxins, and heavy metals are often found in their blood; we also see mast cell activation (specific cells that react to an allergen or other substance, like medication, infection or venom). They tend to have food allergies and what’s called leaky gut, with intestinal hyperpermeability. So it’s not just Lyme that’s making people sick. Lyme is only one part of the problem.”
One of Miller’s friends, a dermatologist, repeatedly told Miller she has CLD; she told Miller she has “all the symptoms.” But Miller’s tests came back negative. Similar to DiFede’s experience, doctor after doctor told Miller there was nothing wrong. Even an infectious disease doctor told Miller she didn’t have Lyme disease, and then this doctor shared that she doesn’t believe in CLD. “I didn’t know they weren’t testing all the bands or for the co-infections,” Miller says.
Unfortunately, the two common Lyme tests (the one you’d receive from a doctor) often fail to accurately diagnose Lyme or CLD. The testing regimen for Lyme disease is a two-tier approach called the ELISA/Western Blot process, which detects Lyme disease by measuring the presence of antibodies that have formed against B. burgdorferi. But, because it can take two to four weeks for the body to generate antibodies, it’s been shown that these tests miss up to 60 percent of acute Lyme cases. Additionally, the test is unable to differentiate between an active infection and previous exposure. “It’s actually not that difficult to diagnose Lyme, but you cannot use the CDC criteria,” says Horowitz. “On their website, they specifically say you don’t want to use the two-tier criteria for an individual diagnosis. It’s mainly meant for health departments to epidemiologically screen large populations of patients. And because there isn’t only one strain of Lyme, testing only one strain won’t provide a complete picture.”
There’s only one place in the country that provides comprehensive testing, IGeneX in California. “It’s the only place that tests all of the eight major strains of Lyme,” Horowitz explains. “They’re considered by many to be the number one testing laboratory.” DiFrede and Miller both received their complete diagnoses from IGeneX via bloodwork that must be shipped overnight. “It’s expensive,” says Miller. “It’s around $2,500 to get all the bloodwork done, and it’s not covered by insurance.” DiFrede’s testing confirmed Lyme, Babesia microti, Bartonella henselae and Mycoplasma. Miller learned she was infected with Lyme, Babesiosis, Bartonella henselae and Ehrlichia.
There are also several clinical markers that can help someone determine if they’re suffering from CLD. “In 2017, I published a validated symptom questionnaire in the International Journal of General Medicine,” says Horowitz. “I worked with doctors Phyllis Freeman and Maryalice Citera at the State University of New York at New Paltz. Before you even do a blood test, the questionnaire can estimate your likelihood of having Lyme disease. It’s now available for free on my website. If you score over 63 on this questionnaire, there’s a very high probability you have chronic Lyme disease.”
The Lyme controversy
CLD is one of the most controversial and vicious medical debates today, but why? With an estimated 476,000 people in the U.S. diagnosed with Lyme annually, according to the CDC, one would think federal dollars would be spent to make better testing and treatment easily available. People are clearly suffering. The honest answer is that it’s complicated, and, depending on who you ask and what you read, it involves various government researchers/departments refusing to admit they were wrong. However, since we’re not ones for conspiracy theories or unproven accusations (even though these make a lot of sense when fully explained), we’ll stick to what we can verify.
Medical schools cannot teach everything, and among the list of what they don’t teach is CLD. Even when a student specializes in infectious disease, they receive no instruction on CLD—they can only learn from studying under a Lyme-literate doctor. In general, the scientific and medical communities are perplexed by how a bacterium can survive in 10 to 30 percent of patients, so how could they possibly teach that in medical school?
“What we learn in medical school is that there’s only one cause for one disease, but Lyme is not caused by one thing,” Horowitz explains. “When you’re dealing with chronic Lyme, you’re dealing with multiple inflammatory factors. That usually is Lyme with Babesia Bartonella, with mold, with metals, with hormone disruption.” In Horowitz’s books (New York Times bestseller, “Why Can’t I Get Better? Solving the Mystery of Lyme and Chronic Disease,” published in 2013, and the national bestseller “How Can I Get Better? An Action Plan for Treating Resistant Lyme and Chronic Disease,” from 2017) and his published research, Horowitz presents a Multiple Systemic Infectious Disease Syndrome (MSIDS) map, which demonstrates that “almost 100 percent of chronic Lyme patients never just have Lyme. They have all these overlapping factors keeping them ill.”
A lack of accurate testing is another issue leading to the controversy. Because the standard two-tier test is so inaccurate, medical professionals wonder how a person can have a chronic bacterial infection that doesn’t show up on tests. Without easily available accurate testing, most doctors are uncomfortable diagnosing and treating a disease they can only speculate about, especially when the symptoms mirror so many other diseases. Lyme, often called “the great imitator,” can look like rheumatoid arthritis, multiple sclerosis, fibromyalgia, chronic fatigue syndrome, Bell’s palsy, PANDAS and more.
And then there’s research, which is either ignored or confuses people. “People from the ‘other side’ who poo-poo chronic Lyme will say there’s no evidence, but there are literally hundreds of articles showing Lyme as a chronic infection,” says Horowitz. “That’s where the politics, unfortunately, interferes with people getting better, and that’s where they’ve misinterpreted these double-blind placebo trials that were done 18 years ago. The results of these trials showed that some people’s fatigue symptoms improved or their memory improved. It also showed that certain co-infections, like Bartonella, could be playing a role. And because some studies showed positive results, while some showed there was no benefit, they have basically sat on the fence and said, ‘We don’t know why people are sick.’”
DiFede wants to be part of the solution. Because she’s spent the majority of her life suffering from CLD, DiFede, who is a junior at Binghamton University, is majoring in neuroscience and hopes to become a physician’s assistant in infectious disease. “But it’s so hard to get into those programs,” she says. “I do well in school, but because I have brain fog, it takes me 100 times more effort than everyone else.”
The confusion over treatment

Miller’s supplies for one day of her IV antibiotic treatment.
When DiFede and Miller were finally properly diagnosed, their Lyme-literate doctors (who often don’t take insurance either) turned to one of the most common treatment options: antibiotics. But these antibiotics come with severe side effects.
“I had a Herxheimer reaction, which is where the antibiotics wake up the bacteria and they say, ‘Something’s killing us! We have to fight,’” DiFede explains. “So my symptoms multiplied by 1,000 percent. I can’t even explain how it feels. I had intravenous antibiotics for three or four weeks, and then I took oral antibiotics for four years.” Many doctors consider IV antibiotics the best course of treatment because they go straight to the blood instead of through the digestive tract. But because insurance doesn’t cover it, patients are forced to do it themselves at home, which can lead to infection.
Miller recently began IV antibiotics after having a vascular surgeon install a port through her jugular vein. “It had to heal for a couple of weeks before I could begin antibiotics,” Miller explains. “Then, a nurse came to my house to install the final piece and train me. My daily treatment begins by flushing the line to make sure there’s no air in the line. It’s very stressful and scary to do this myself, and I break out in a big sweat. If I mess it up, I could die. Then, I take two different antibiotics, and they take about 30 minutes each to fully drip into my body. Finally, I have to flush out the line for another couple of minutes.” Miller hasn’t noticed a positive difference with the IV antibiotics yet, and she says she won’t truly know if the antibiotics have worked until her treatment cycle is complete in mid-June. Miller says the only treatment that has brought her any relief is her monthly eight-hour immunoglobulin infusion treatments, which she began in September. She says she feels better for three weeks before feeling awful again.
And now, Miller is experiencing Herxheimer reactions from the antibiotics, which are debilitating some days and nonexistent on others. These reactions are par for the course, and they can continue for weeks or months with IV and even longer with oral antibiotics. “My doctor told me it’s definitely going to get a lot worse, but you have to push through it to get better,” DiFede remembers. “It was awful, and for years my mental state was horrible. I would go to bed and pray I wouldn’t wake up. When I did wake up, I would just cry, thinking ‘this again?’ But then, I woke up one morning, and it was just gone. And I was so happy. I thought it would never end. It was two years of wanting to kill myself or wishing I would die every day, and then it was just gone.”
Now, unfortunately, two and a half years after she completed her antibiotics, many of DiFede’s symptoms have returned, including the brain fog. Her desire to feel healthy again led her to explore a treatment center in Germany called Clinicum St. Georg where they employ a treatment called systemic whole-body hypothermia. “They knock you out and boil your body for about seven hours and then bring you back to,” McEneaney, DiFede’s mom, explains. “And you do that for about a week.” DiFede adds, “They literally heat your body to 108 degrees for seven hours. So you could die; your organs could fail. They have a doctor monitoring you the entire time, and I don’t think anyone has died, but it’s scary. It takes several months for your body to recover, and some people never have a symptom again; they are cured. But for other people, it comes back in a year.”Considering the cost (ranging from $20,000 to $30,000) and the uncertain outcomes, DiFede and McEneaney decided to hold off on the treatment for now. But they still think about it.
Horowitz, however, has discovered a different form of treatment, which he’s extensively researched and published numerous papers about. He’s found that dapsone, a sulfur-based drug originally used to treat leprosy, can effectively cure CLD, even clearing out what many believe is permanent brain fog. “That’s the number one symptom that gets better,” he says. To understand why this treatment works, it’s important to understand leprosy. “Leprosy is a slow-growing intracellular bacteria that’s difficult to treat,” Horowitz explains. “It takes a year of rifampin and dapsone, which is how I came up with this protocol. Dapsone has great penetration into the brain. It’s antimalarial and also anti-inflammatory, which can help people that have autoimmune reactions. The truth is, it’s a fabulous drug.”
But like any drug, it does have side effects. Over the years, Horowitz has figured out how to “reverse” those side effects. His nine-week protocol requires a double dose of dapsone as well as doxycycline and rifampin, all generic medications available at your local pharmacy. And once treatment is complete, CLD is gone. “This is not something they have to live with for the rest of their lives,” he says. “But the main thing that interferes with the success of the protocol is mold. We find that if we don’t get rid of the mold toxins, people do not respond adequately.”
His next step is to conduct a randomized, multicenter, placebo-controlled trial on dapsone, and he’s applied for the R34 NIH grant to conduct his study. “That is the gold standard for me to prove to the world that I have discovered an answer,” he explains. “Until that happens, there are many doctors who use different treatments, and some of it does help. My concern is that I want it quick. I want it fast, and I don’t want it to be expensive.” In the meantime, he’s trained “hundreds and hundreds of doctors” on this model, and the exact treatment regimen is available online for anyone to use. “Not everybody’s doing the protocol,” he says. “Some are worried about the side effects of dapsone. They should be more worried about the side effects of this infection for the rest of people’s lives.”
There is hope
Years ago, a vaccine was developed for Lyme but removed from the market due to side effects. In July 2024, Pfizer and Valneva completed their Phase 3 trial of a vaccine called VLA15 and plan to monitor participants for Lyme disease until “the end of the Lyme disease season in 2025.” Horowitz is hopeful, but his one concern is that the vaccine hasn’t been tested in people with Lyme, and he is concerned those who unknowingly have Lyme in their system may experience extreme side effects.
“There’s also a vaccine in the works by Mark Klempner from Tufts,” says Horowitz. “It’s basically a monoclonal antibody that gives you protection for a year. And Dr. Utpal Pal is researching a tick spit vaccine so that the minute the tick attaches, you have antibodies, and the tick falls off. There are many things people are working on, but the one that will probably be released earliest is the VLA15.”
A preventive vaccine and a proven cure would change the lives of hundreds of thousands. “I’m not as sharp as I used to be, and I don’t like it,” says Miller. “I don’t like not being the smartest one in the room; that’s what I’m used to. It feels good when you’re well-read and you know your stuff. I love the feeling of being strong, physically and mentally, and to have that taken away is really hard.
This article was published in the May/June 2025 edition of Connect to Northern Westchester.

Gia Miller is an award-winning journalist and the editor-in-chief/co-publisher of Connect to Northern Westchester. She has a magazine journalism degree (yes, that's a real thing) from the University of Georgia and has written for countless national publications, ranging from SELF to The Washington Post. Gia desperately wishes schools still taught grammar. Also, she wants everyone to know they can delete the word "that" from about 90% of their sentences, and there's no such thing as "first annual." When she's not running her media empire, Gia enjoys spending quality time with friends and family, laughing at her crazy dog and listening to a good podcast. She thanks multiple alarms, fermented grapes and her amazing husband for helping her get through each day. Her love languages are food and humor.

Justin is an award-winning designer and photographer. He was the owner and creative director at Future Boy Design, producing work for clients such as National Parks Service, Vintage Cinemas, The Tarrytown Music Hall, and others. His work has appeared in Bloomberg TV, South by Southwest (SXSW), Edible Magazine, Westchester Magazine, Refinery 29, the Art Directors Club, AIGA and more.
Justin is a two-time winner of the International Design Awards, American Photography and Latin America Fotografia. Vice News has called Justin Negard as “one of the best artists working today.”
He is the author of two books, On Design, which discusses principles and the business of design, and Bogotà which is a photographic journey through the Colombian capital.
Additionally, Justin has served as Creative Director at CityMouse Inc., an NYC-based design firm which provides accessible design for people with disabilities, and has been awarded by the City of New York, MIT Media Lab and South By Southwest.
He lives in Katonah with his wonderfully patient wife, son and daughter.