
By Gia Miller
Photography by Justin Negard
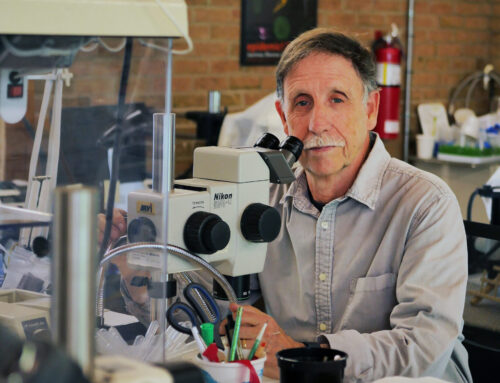
“I’ll never forget that feeling of driving into the city when I knew everybody else was leaving it,” says Katonah resident Dr. Rituparna Pati, M.D. “Being there felt kind of apocalyptic.”
It was March of 2020, and Pati raised her hand. As an infectious disease physician and medical epidemiologist with the Centers for Disease Control and Prevention (CDC), she had the knowledge, skills and resources, and she felt “compelled” to help. The New York City Department of Health and Mental Hygiene (DOH) accepted Pati’s offer, asking her to lead the infection prevention and control team at the Jacob Javits Convention Center, which had been converted into an alternate care facility to manage the hospitals’ overflow of COVID-19 patients.
“I actually rented an apartment in Manhattan for six weeks so I could be nearby and limit the exposure to my family,” she remembers. “And within the first couple days, I realized that I was the only infectious disease physician on the ground amongst the approximately 700 federal workers at Javits, and I was the only one from the CDC as well.”
“There were phenomenal physicians and medical experts from agencies including the Army, the National Guard, the Reserves, FEMA, the U.S. Public Health Service and the New York City DOH —this was a true multi-agency effort,” she continues. “And I just felt that being in that role really brought together all my years of training and work experience. I knew how to navigate that type of multi-agency environment; I knew how to communicate technical points in a compelling way that’s easily understood; and I knew about infection prevention and control as well as epidemiology. Everything led to that moment. It was obviously a very stressful time, and I wouldn’t want to wish a pandemic on any of us, but it was also a very fulfilling work experience.”
Pati worked 12-15 hours a day, setting guidelines to protect healthcare workers (mask mandates, PPE, etc.), implementing protocols to prevent patients from infecting one another, and even creating staff screening policies like temperature checks and symptom tracking.
“I remember distinctly coming up with an algorithm for how to screen patients who are transferred to ensure they’re not potentially exposing patients to other infections,” she explains. “Just because COVID was happening, it didn’t mean that measles or TB suddenly stopped or went away. So, we had to think about these things before bringing patients from other settings into this very potentially vulnerable space.”
But even though she expertly implemented measures that saved countless lives, highly contagious airborne diseases are not Pati’s specialty. She’s spent her career focusing on the global AIDS epidemic. In fact, she’s currently “on loan” from the CDC to the federal government, working as a senior technical advisor for HIV care and treatment within the Office of Program Quality at the Bureau of Global Health Security and Diplomacy (GHSD)—The United States President’s Emergency Plan for AIDS Relief (PEPFAR).

A map in Pati's home that shows the many countries she has traveled to.
Desire to make an impact
Pati chose a career in medicine because she wanted to “have a voice and make a population-level impact.” She felt a calling to work in public health, so she earned a combined medical and master’s of public health degree from the University of Connecticut. And during her second year, she had her “aha” moment.
“Our entire class filed into the auditorium to watch a documentary on the global HIV epidemic,” Pati remembers. “It was 2002, and at that time, more than 8,000 people were dying of HIV/AIDS every day. I heard that figure, and I just felt like that was unacceptable. I wanted to do something about it. From that moment on, I worked towards developing the skills and finding opportunities to contribute to curbing the devastating effects of HIV.”
“At that point, we had effective treatments for HIV in the U.S.,” she continues. “So, I knew this was an issue of access, of getting that reach into other parts of the world where people did not yet have access to these lifesaving medications.”
Pati completed her internal medicine residency at NewYork-Presbyterian/Weill Cornell Medical Center in Manhattan, and because she wasn’t sure if she wanted to specialize in infectious disease, she went to work as a general medicine attending physician at Bellevue Hospital. One year later, former mentors from her residency reached out, offering Pati an opportunity to join their infectious disease fellowship, and she accepted. While there, Pati served as a primary care provider for HIV patients and, as part of her fellowship, completed a preventive medicine residency program, developing expertise in disease prevention, implementation science and epidemiologic research.
Next, Pati became the director of research at the Spencer Cox Center for Health at Mount Sinai St. Luke’s Roosevelt, which was the largest HIV clinical care center in the state. For two years, she conducted research and developed a new research division before moving to Atlanta to work as a medical officer at the CDC.

Pati joined this vaccination team in a door-to-door polio vaccination campaign in Lusaka, Zambia. Photo courtesy of Dr. Rituparna Pati.
Curbing an epidemic
When Pati began at the CDC in the fall of 2014, she remained focused on HIV, but her work was on a global scale across a wide range of countries served by PEPFAR. And she served as the point of contact for the African countries of Namibia and Tanzania.
“In my initial years, I was really involved in launching the first HIV Project ECHO in Africa, which is a video conferencing platform that serves as a form of mentorship for providers,” Pati explains. “It’s a hub and spoke model where you have a hub of experts who use a video conferencing platform to connect to providers in very remote areas to offer their expertise. It’s really a case-based learning model to support these healthcare providers, who are working in pretty challenging circumstances in very remote conditions. We launched it in Namibia as an example for other countries to follow.”
During her nine years with the CDC, Pati worked her way up to supervising a team of CDC medical officers, epidemiologists and health scientists, as well as collaborating with agencies around the globe. Pati had two main missions: increase HIV viral load testing and optimize treatment regimens.
“I was looking at the clinical and laboratory interface and how that can be strengthened to ensure access to viral load testing for all people living with HIV,” she explains. “I also focused on optimizing treatment regimens, which was a major effort because PEPFAR went through a transition several years ago to a new first line treatment regimen. So that meant transitioning more than 15 million people over to a new first line therapy, which, of course, is a huge effort. And while I was a CDC representative on that effort, it really involved a lot of interagency work that spans across countries.”
While Pati could do a lot of work from her office in Atlanta and later Katonah—she moved back to New York in 2017—international trips, which occurred every other month, were a requirement. She says her field visits to Namibia and Tanzania were especially memorable because she returned to those countries year after year.
“So much of the work that we do is about relationships,” she explains. “Over the years, I developed a very close relationship with the physicians who were working in Namibia and Tanzania as part of the PEPFAR team and the laboratory branch of the CDC in those countries. It was a very multidisciplinary effort, so I really got to know people across that CDC team, including laboratory scientists, strategic information officers, the country directors, USAID (Agency for International Development) and the Department of Defense.”
Several times a year, Pati would make the approximately 20-hour, week-long trip from her home in Katonah to her hotel in Namibia or Tanzania to conduct site visits. Pati would arrive on a Sunday evening and awake before dawn the next morning. She, and often a team, would begin their day by traveling three to four hours over bumpy roads to their first appointment, often a regional director for the Ministry of Health. They’d discuss their plan, receive the necessary clearance, and then visit the care and treatment site in that area.
“Each trip had a specific focus,” Pati explains. “For example, if the goal was to focus on viral load, we would assess the flow of the clinic, then what was happening in the laboratory, and how the results would be shared back to the clinic. How do they order a test? How does the patient know where to go? How do the results get back to the provider? But if I was looking at antiretroviral regimen optimization, then it was very different. We would look at what kind of protocols were in place at the clinic. Were providers following them to transition a patient to the new regimen? We would review the records to see which patients had already started the new regimen and how they are being tracked. Did they have consent forms for the patients? But then, of course, there were certain visits where we did look at everything from A to Z.”
These site visits took several hours, and, depending on the region, Pati would often visit two or three, sometimes four, sites each day. Then, when she traveled with a team, they would debrief over dinner at their small hotel, discussing what went well and how they could improve their approach the next day to get all the information they needed.
“It was exhausting, physically and mentally,” she says. “But while it was strenuous and rigorous, the work overall was fulfilling. And the most fulfilling aspect of the work was spending that time in the country with the team. Even though it was hard to be away from family and to be jet lagged, feeling connected to the people that you’re serving and actually seeing the sights and how care is being delivered was really the most fulfilling.”

A district hospital in Djoum, Cameroon that also serves as an HIV Care and Treatment site. Photo courtesy of Dr. Rituparna Pati.
Making global change
Pati began her long-term detail with GHSD-PEPFAR in August of last year; she expects it will last approximately two years.
“PEPFAR is a congressionally funded program that was launched in 2003 as an emergency response to the large number of deaths happening around the world due to HIV,” she explains. “It’s a multi-agency, federal government effort that includes the CDC, USAID, NIH [National Institutes of Health], Department of Defense, Department of Health and Human Services, HRSA [Health Resources and Services Administration] and the Peace Corps. And my essential function is to serve as a technical advisor for the quality of the HIV care and treatment programs that we support around the world.”
“We’re using all the scientific evidence that we have available to provide evidence-based recommendations, optimal treatment regimens, optimal prevention options and a combination prevention approach,” Pati continues. “We’re putting our best effort forward in terms of preventing the transmission of HIV and, for those who are infected with HIV, ensuring that they are diagnosed early and started on treatment as soon as possible so they can live the longest, healthiest life that we’re able to provide.”
There are regular inter-agency data reviews of PEPFAR’s programs to ensure their local partners on the ground are doing the work and providing the care and services required.
“We look at how many people have been newly diagnosed and if it matches expectations,” Pati explains. “We look at how many people have recently started treatment. Are they covering certain gaps in certain populations? Have they reached full coverage? And then, how many people have achieved viral load suppression? And that’s really our ultimate outcome; we’re working towards getting as many people living with HIV as possible suppressed, meaning the HIV virus is undetectable, they can’t transmit it to others and they can live their full lifespan.”
One of the ways Pati hopes to do this is by addressing other health conditions for people living with HIV. She is leading an initiative that will explore models and collect data to determine the effectiveness of programs that integrate hypertension services with HIV services.
For example, she’ll examine whether people will access HIV treatment services more because they know they will also receive hypertension treatment. Will they stay in treatment longer, and therefore stay virally suppressed, because their other health needs are being met?
The HIV Coverage, Quality, and Impact Network (CQUIN), led by Columbia University and funded mainly by the Bill & Melinda Gates Foundation, recently organized a meeting in Nairobi, Kenya, at which Pati was invited to speak about this topic.
“CQUIN brings representatives from the ministries of health in 21 different countries,” Pati explains. “They’re really focused on learning from each other about the different models of service delivery for people living with HIV. The focus of this meeting was specifically on integrating other services with HIV services. One day was focused on hypertension services with HIV, and another day was focused on family planning services with HIV. So, I spoke about PEPFAR’s new initiative and that we are interested in learning and exploring with them. It was wonderful, and I was fortunate to be invited and be part of that discussion.”
Although she now travels for speaking engagements every few months and is focused on global care, she still connects to our community by volunteering some of her time to provide care to HIV patients at the James J. Peters VA Medical Center in the Bronx, which she’s done since 2018.
“I do it to stay clinically active and up to date with managing HIV,” Pati explains. “I was a volunteer physician at the Atlanta VA Medical Center when I lived there. Many infectious disease physicians who work at the CDC try to incorporate clinical practice into their work schedules for that reason. For me, working with patients to some degree helps keep me grounded in the work that we do at PEPFAR.”

Baby with a finger marked to show vaccination status. Photo courtesy of Dr. Rituparna Pati.
What she wants you to know
“A lot of people don’t realize that some of the countries we support have better control of the HIV epidemic than we do in the U.S.,” says Pati. “Countries have achieved epidemic control when 95 percent of people with HIV are aware of their diagnosis, 95 percent of those diagnosed are on treatment and 95 percent of those who are on treatment are virally suppressed. We have several countries that have reached that benchmark; the U.S. has not.”
“HIV is no longer a death sentence,” she continues. “We have very effective, very well-tolerated medicines that, if people start treatment early enough, meaning soon after diagnosis, they can live a totally normal lifespan.”
But you must get tested, Pati stresses, noting that the recommendation is for everyone ages 13 to 64 to get tested for HIV at least once during their routine health examination. And if you’re engaging in behaviors that increase transmission (like an exchange of bodily fluids or sharing needles), you should get tested more often, and, importantly, modify your behaviors to prevent infection.
“We’ve come a long way,” says Pati. “In addition to behavioral methods of prevention, now there are also biomedical modes of prevention for people who are high-risk. There’s a daily pill, a vaginal ring or a bi-monthly shot that will protect you from HIV. But in so many parts of the world, including the U.S., a big gap is that people don’t know their status, and they need to get tested for HIV. Because if you don’t know you’re infected, you can pass it on to others. And there’s still a lot of stigma associated with HIV, even though there shouldn’t be. We continue to work towards minimizing the stigma associated with HIV, but again, people need to get tested.”
Pati dreams of the day when scientists discover a vaccine that provides lifelong protection against HIV, resulting in the eventual eradication of the virus.
“It’s been decades of research,” she says. “And the sad part is that nothing has proven to be effective yet. So much talent and resources continue to go towards trying to find a vaccine, but this virus is a tough one. It’s a really tricky virus.”
Pati’s other dream, her personal one, is to live and work overseas for a few years.
“I would love for my son to experience living overseas for a couple of years and for all of us to experience a new culture and lifestyle together as a family.”

Children gathering to receive an oral polio vaccine and have their finger marked after vaccination. Photo courtesy of Dr. Rituparna Pati.
This article was published in the July/August 2024 edition of Connect to Northern Westchester.

Gia Miller is an award-winning journalist and the editor-in-chief/co-publisher of Connect to Northern Westchester. She has a magazine journalism degree (yes, that's a real thing) from the University of Georgia and has written for countless national publications, ranging from SELF to The Washington Post. Gia desperately wishes schools still taught grammar. Also, she wants everyone to know they can delete the word "that" from about 90% of their sentences, and there's no such thing as "first annual." When she's not running her media empire, Gia enjoys spending quality time with friends and family, laughing at her crazy dog and listening to a good podcast. She thanks multiple alarms, fermented grapes and her amazing husband for helping her get through each day. Her love languages are food and humor.